ANAEMIA

Hey all...

Hey all...
I shall take you through a very important topic tonight..
Anaemia/Anemia

It is the most common disorder globally and one of the conditions that general practitioners most frequently encounter. In the World Health Organization global database, anaemia is estimated to affect 1.6 billion people. As anaemia manifests in a wide range of conditions, it is important to embrace a structured diagnostic approach...
Below is the outline for the presentation...
*DEFINITION*Anaemia/Anemia
It is the most common disorder globally and one of the conditions that general practitioners most frequently encounter. In the World Health Organization global database, anaemia is estimated to affect 1.6 billion people. As anaemia manifests in a wide range of conditions, it is important to embrace a structured diagnostic approach...
Below is the outline for the presentation...
-Outline
-Definition
-Classification
-Effect
-Pharmacology
Anaemia is defined as a condition in which the number of red cells or their oxygen-carrying capacity is insufficient to meet physiological needs. ie _decrease the RBCs count or Hb content or both below the normal range for age and sex_
➖According to the World Health Organization (WHO), anaemia is defined as ‘a condition in which the number of red blood cells or their oxygen-carrying capacity is insufficient to meet physiologic needs’. Anaemia is rarely an isolated disease and is most often a sign of an acquired or inherited disorder.According to the WHO global database, anaemia is estimated to affect 1.6 billion people. The highest prevalence is found in preschool-age children (47.4%), followed by pregnant females (41.8%), non-pregnant females (30.2%), school-age children (25.4%), and males (12.7%).
Red cells are produced in the bone marrow (BM) from myeloid progenitor cells, where their production requires a permissive bone marrow micro-environment and adequate substrate (including iron, vitamin B12 and folate) for Hb, protein and DNA synthesis.
Erythropoiesis is controlled by erythropoietin (EPO), which is synthesised by peritubular fibroblasts in the renal cortex in response to reduced oxygen tension.
*CLASSIFICATION*
Anaemia may be classified under two criteria
1.Base on the RBC characteristics and
2. Base on the cause
Anaemia may be classified under two criteria
1.Base on the RBC characteristics and
2. Base on the cause
Let start with the first one...
*1.Based on red cell characteristics*
( _size of RBCs and to the Hb content in each RBC and morphology_), it can be classified into the following
( _size of RBCs and to the Hb content in each RBC and morphology_), it can be classified into the following
*(A)Normocytic/Normochromic Anemia*:
the RBCs size is normal (Normocytic) and the Hb content in each RBC is normal (Normochromic).
*(B).Microcytic/Hypochromic Anemia*:
the RBCs size is below the normal (Microcytic)
and the Hb content in each RBC is decreased (Hypochromic).
it is due to deficiency of iron, so it is called (iron deficiency anemia).
*C). Macrocytic hyperchromic anemia* (megaloblastic anemia):
the RBCs size is above the normal (macrocytic) and the Hb content in each RBC is increased (hyperchromic).
It is due to deficiency of vitamin B12 or folic acid.
the RBCs size is above the normal (macrocytic) and the Hb content in each RBC is increased (hyperchromic).
It is due to deficiency of vitamin B12 or folic acid.
*(A) Normocytic Normochromic anemia*:
the RBCs size is normal (Normocytic) and the Hb content in each RBC is normal (Normochromic).
CAUSES OF Normocytic Normochromic anemia 👇🏿👇🏿
1- *Hemolysis of RBCs* (hemolytic anemia): it may be due:
a- Intravascular (IV) causes: This include the following
a- Intravascular (IV) causes: This include the following
i- Cell membrane defect [e.g. hereditary spherocytosis].
ii- Hb defect [e.g. sickle cell anemia, thalassemia (α &β)].
iii- Enzymatic defect [Glucose 6 phosphate dehydrogenase deficiency (favism)].
ii- Hb defect [e.g. sickle cell anemia, thalassemia (α &β)].
iii- Enzymatic defect [Glucose 6 phosphate dehydrogenase deficiency (favism)].
b- Extravascular (EV) causes:
i- Drugs.
ii- Snake venoms.
iii- Bacterial toxins.
i- Drugs.
ii- Snake venoms.
iii- Bacterial toxins.
2- *Acute blood loss* (Hemorrhagic anemia).
3- *Bone marrow depression*(Aplastic anemia): it may occur in:
i- Excessive exposure to radiation (e.g. X-ray).
ii- Some viral infections.
iii- Some drugs (e.g chemotherapy).
iv- Invasion of bone marrow by malignant cells.
i- Excessive exposure to radiation (e.g. X-ray).
ii- Some viral infections.
iii- Some drugs (e.g chemotherapy).
iv- Invasion of bone marrow by malignant cells.
*(B). Microcytic Hypochromic anemia*:
• the RBCs size is below the normal (Microcytic)
and the Hb content in each RBC is decreased (Hypochromic).
• the RBCs size is below the normal (Microcytic)
and the Hb content in each RBC is decreased (Hypochromic).
it is due to deficiency of iron, so it is called (iron deficiency anemia).
CAUSES👇🏿👇🏿
1- ↓ iron intake: as in malnutrition or starvation.
2- ↓ absorption: it may be due to:
a- ↓ reducing agents [e.g. HCl & vitamin C].
b- Presence of phytic acid (in tea), phosphate or oxalate in food.
c- ↓ bile (because it contains apotransferrin that is necessary for absorption).
a- ↓ reducing agents [e.g. HCl & vitamin C].
b- Presence of phytic acid (in tea), phosphate or oxalate in food.
c- ↓ bile (because it contains apotransferrin that is necessary for absorption).
3- Chronic blood loss: this is could be because of:
a- GIT bleeding (e.g. peptic ulcer or piles).
b- Hematuria.
c- Excessive menstruation (most common cause of anemia in females).
a- GIT bleeding (e.g. peptic ulcer or piles).
b- Hematuria.
c- Excessive menstruation (most common cause of anemia in females).
4- ↓ storage [as in liver diseases].
5- ↑ requirements [as in pregnancy, lactation, and rapid growth in puberty].
*C). Macrocytic hyperchromic anemia* (megaloblastic anemia):
the RBCs size is above the normal (macrocytic) and the Hb content in each RBC is increased (hyperchromic).
It is due to deficiency of vitamin B12 or folic acid.
CAUSES 👇🏿👇🏿
1- ↓ intake [malabsorption or starvation].
2- ↓ absorption: it could be due to:
a- ↓ IF due to atrophy of gastric mucosa (called pernicious anemia).
a- ↓ IF due to atrophy of gastric mucosa (called pernicious anemia).
b- Disease or excision of the terminal ileum (absorption site).
3- ↓ storage [as in liver diseases].
_morphologically we have_
• leuco-erythroblastic
• micro-/macroangiopathic.
• leuco-erythroblastic
• micro-/macroangiopathic.
*2). CLASSIFICATION ACCORDING TO THE CAUSE*
*(1) Hemorrhagic anemia* :
This is anemia caused by acute or chronic blood loss (e.g. due to bleeding peptic ulcers or piles.
This is anemia caused by acute or chronic blood loss (e.g. due to bleeding peptic ulcers or piles.
*(2) Hemolytic anemia* :
This is anemia caused by excessive hemolysis (breakdown) of the R.B.C.s. Hemolysis may occur due to either :
(a) lntracapsular (congenital) causes e.g. abnormalities in the red cell membranes (as in congenital spherocytosis) or in Hb (as in sickle cell anemia and thalassemia) or deficiency of the G6PD enzyme.
(b) Extracapsular (acquired) causes e.g. certain drugs, chemicals and toxins (as some snake venoms). certain infections. malaria. hyper-splenism, incompatible blood transrusion and autoimmunity (i.e. formation of abnormal antibodies that attack the red blood cells).
This is anemia caused by excessive hemolysis (breakdown) of the R.B.C.s. Hemolysis may occur due to either :
(a) lntracapsular (congenital) causes e.g. abnormalities in the red cell membranes (as in congenital spherocytosis) or in Hb (as in sickle cell anemia and thalassemia) or deficiency of the G6PD enzyme.
(b) Extracapsular (acquired) causes e.g. certain drugs, chemicals and toxins (as some snake venoms). certain infections. malaria. hyper-splenism, incompatible blood transrusion and autoimmunity (i.e. formation of abnormal antibodies that attack the red blood cells).
*(3) Aplastic anemia* :
This is anemia caused by damage of the bone marrow e.g. due to
(a) exposure to excessive x ray or gamma ray radiation
This is anemia caused by damage of the bone marrow e.g. due to
(a) exposure to excessive x ray or gamma ray radiation
(b) Certain drugs {e.g. chloramphenicol) and chemicalls (e.g. arsenic)
(c) Leukemia (in which the excessively-proliferating white cells in the bone marrow decrease red cell formation)
(d) Certain chronic infections.
*(4) Nutritional (deficiency) anemias* :
This is anemia caused by deficiency of the nutritional factors that are required for erythropoiesis e.g. :
(a) Anemia due to deficient supply of iron (iron deficiency anemia).
(b) Pernicious anemia (due to vitamin B12 deficiency).
(c) Macroctyic anemia (due to folic acid deficiency).
This is anemia caused by deficiency of the nutritional factors that are required for erythropoiesis e.g. :
(a) Anemia due to deficient supply of iron (iron deficiency anemia).
(b) Pernicious anemia (due to vitamin B12 deficiency).
(c) Macroctyic anemia (due to folic acid deficiency).
*EFFECTS OF ANEMIA*
(Reduction of the blood viscosity and O2 lack. The former decreases the peripheral resistance while the latter causes V. D. Both effects increase the venous return and consequently the cardiac output, which increases the work load on the heart.
(2) Increase of the blood velocity (due to reduction of viscosity) and this increases the blood turbulence which accentuates the heart sounds and may produce functional murmurs.
(3) Decrease of the O2 content in the arterial blood which leads to tissue hypoxia and rapid fatigue.
*CLINICAL MANIFESTATION*
– Pallor
– Palpitation
– Fatigue
– Fainting
– Headache
– Blurring of vision].
– Pallor
– Palpitation
– Fatigue
– Fainting
– Headache
– Blurring of vision].
_In order to properly treat the anemia, you must determine the cause
When investigating patients with anaemia, two fundamental questions have to be considered:
(i) What is the cause of the anaemia
(i) What is the cause of the anaemia
(ii) What is the urgency for correcting the anaemia, i.e. is a blood transfusion or other urgent intervention indicated?
PHARMACOLOGY 👇🏿👇🏿
We will start with
*1. Iron deficiency anemias*
*Therapeutic uses of Iron*- in
Iron Deficient Anemia,
¤ Pregnancy,
¤ Premature Babies,
¤ Blood loss,
¤ Hookworn infestation,
¤ Malabsorption Syndrome,
¤ GI Bleeding due to:
~ Ulcers
~Aspirin
¤ Excess consumption of coffee
*Iron salt supplements*
Iron Deficient Anemia,
¤ Pregnancy,
¤ Premature Babies,
¤ Blood loss,
¤ Hookworn infestation,
¤ Malabsorption Syndrome,
¤ GI Bleeding due to:
~ Ulcers
~Aspirin
¤ Excess consumption of coffee
*Iron salt supplements*
*a. Oral agents*
(1) Several ferrous iron salts are available for oral use. All are essentially equivalent therapeutically if doses are adjusted according to iron content (gluconate, sulfate, and fumarate forms are 12%, 20%, and 33% iron by weight, respectively; a polysaccharide–iron complex is also available).
(2) Approximately 25% of orally administered iron is absorbed; a typical daily dose is 100–200 mg iron/day.
(3) Oral iron treatment may require 3–6 months to replenish body stores.
*b. Parenteral agents*
*b. Parenteral agents*
(1) A colloidal suspension of ferrous hydroxide and dextran can be administered by intravenous (IV) infusion or intramuscular injection.
(2) Parenteral agents may be useful in patients with iron absorption disorders caused by inflammatory bowel disease, small-bowel resection, gastrectomy, or hereditary absorption defects.
(3) Parenteral agents are indicated for patients with hypersensitivity reactions to oral iron salts.
(4) These agents are useful in severe anemic conditions in which rapid correction of iron deficiency is desired.
(5) Parenteral agents may be used to reduce toxic reactions on initiation of erythropoietin (EPO; epoetin alfa) therapy in patients with renal disease.
*c. Adverse and toxic effects*
(1) Iron salt supplements produce gastrointestinal (GI) upset (nausea, cramps, constipation, and diarrhea).
*c. Adverse and toxic effects*
(1) Iron salt supplements produce gastrointestinal (GI) upset (nausea, cramps, constipation, and diarrhea).
(2) These supplements may cause hypersensitivity reactions (most common with parenteral administration), including bronchospasm, urticaria, and anaphylaxis.
(3) Fatal iron overdose (1–10 g) is possible; children are especially susceptible. Deferoxamine (Desferal), an iron-chelating agent, is used to treat iron toxicity. Administered systematically or by gastric lavage, deferoxamine binds iron and promotes excretion.
*Toxicity of Iron Overdose* :At high doses, Iron is absorbed through passive diffusion with no regulation and has led to death of many..
Next is
*2. Red cell deficiency anemias*
1.Red cell deficiency anemias are most commonly treated with erythropoiesis-stimulating agents (ESAs).
In addition to ESAs above, we have
*2. EPO (Epogen, many others)*
*2. EPO (Epogen, many others)*
We shall briefly talk on EPO next...
*a. Properties*
*a. Properties*
(1) EPO is a glycoprotein produced mostly (90%) by the peritubular cells in the kidney; EPO is essential for normal reticulocyte production.
(2) Synthesis of EPO is stimulated by hypoxia
(3) EPO is available as recombinant human EPO, epoetin alfa, and darbepoetin. Darbepoetin is a second-generation ESA with a half-life about twice that of epoetin alfa. *Administered parenterally (IV or subcutaneously).*
*b. Mechanism of action*
(1) EPO increases the rate of proliferation and differentiation of erythroid precursor cells in the bone marrow.
(2) EPO induces the transformation of the most mature erythroid progenitor cell, erythroid colony-forming unit, to a proerythroblast.
(3) EPO increases the release of reticulocytes from marrow.
(4) EPO increases hemoglobin synthesis.
(5) The action of EPO requires adequate stores of iron.
(1) EPO increases the rate of proliferation and differentiation of erythroid precursor cells in the bone marrow.
(2) EPO induces the transformation of the most mature erythroid progenitor cell, erythroid colony-forming unit, to a proerythroblast.
(3) EPO increases the release of reticulocytes from marrow.
(4) EPO increases hemoglobin synthesis.
(5) The action of EPO requires adequate stores of iron.
*Therapeutic uses*.
EPO is used to treat anemia in the following patients:
➖acquired immune deficiency syndrome patients treated with zidovudine (AZT)
EPO is used to treat anemia in the following patients:
➖acquired immune deficiency syndrome patients treated with zidovudine (AZT)
➖cancer patients undergoing chemotherapy, and
➖patients in renal failure; _all of these conditions and treatments produce anemia_.
➖patients in renal failure; _all of these conditions and treatments produce anemia_.
EPO is also used in surgical patients to reduce the need for transfusions. In a situation requiring a rapid increase in hematocrit, RBC transfusion is effective in 1–3 hours while EPO takes 2–6 weeks.
*d. Adverse and toxic effects of EPO* include hypertension, seizures, and headache probably caused by rapid expansion of blood volume. ESAs have been shown to increase the risk of death and serious cardiovascular events, both arterial and venous thromboembolic events including myocardial infarction (MI), stroke, congestive heart failure, and hemodialysis graft occlusion, when administered to target a hemoglobin concentration of 12 g/dL.
We now move to the next group of anemias....
*3.) Sideroblastic anemias*
1. Sideroblastic anemias are characterized by decreased hemoglobin synthesis and intracellular accumulation of iron in erythroid precursor cells. Iron is available but is not incorporated into hemoglobin in a normal manner.
2. Sideroblastic anemias are often caused by agents that antagonize or deplete pyridoxal phosphate.
3. Sideroblastic anemias are sometimes seen in alcoholics, in patients undergoing anti-tuberculin therapy with isoniazid and pyrazinamide, and in certain inflammatory and malignant disorders.
4. Hereditary sideroblastic anemia is an X-linked trait.
5. *Sideroblastic anemia is treated with pyridoxine (vitamin B6) administered orally (preferred route) or parenterally. Pyridoxine has variable efficacy with inherited forms of the disease*
Next is a very common type...
*4.Vitamin deficiency (megaloblastic) anemia*
*1.Vitamin B12*
*Source:* In food, especially in liver and kidneys. GI Microorganism synthesis, Vitamin Supplements (Cyanocobalamin)Necessary for normal DNA synthesis,
*1.Vitamin B12*
*Source:* In food, especially in liver and kidneys. GI Microorganism synthesis, Vitamin Supplements (Cyanocobalamin)Necessary for normal DNA synthesis,
*Absorption of B12*
1. Intrinsic Factor (low dose): a protein made by stomach parietal cells that binds to B12 and delivers it from the ileum via a calcium mediated event.
2. Mass Action (High dose): 1000mg/day, absorbed via passive diffusion
*B12 DEFICIENCY*
A B12 deficiency will cause peripheral neuropathy and a macrocytic anemia, a pernicious anemia. Folic Acid administration can correct the macrocytic anemia but will fail to correct the peripheral neuropathy. To treat the neuropathy, Vit B12 must be utilized
(1) Vitamin B12 is essential for normal DNA synthesis and fatty acid metabolism. A deficiency results in impaired DNA replication, which is most apparent in tissues that are actively dividing, such as the GI tract and erythroid precursors. The appearance of large macrocytic (megaloblastic) red cells in the blood is characteristic of this deficiency. Vitamin B12 deficiency can also result in irreversible neurologic disorders.
(2) Vitamin B12, along with vitamin B6 and folic acid, participates in the metabolism of homocysteine to cysteine. Elevations in homocysteine are associated with accelerated atherosclerosis.
(3) Loss of vitamin B12 from the body is very slow (2 μg/day), and hepatic stores are sufficient for up to 5 years. Vitamin B12 is not synthesized by eukaryotic cells and is normally obtained from microbial synthesis.
(4) Parenteral administration of vitamin B12 is standard because the vast majority of situations requiring vitamin B12 replacement are due to malabsorption. Uncorrectable malabsorption requires life-long treatment.
(5) Improvement in hemoglobin concentration is apparent in 7 days and normalizes in 1–2 months.
*Therapeutic uses*
(1) Vitamin B12 is used to treat pernicious anemia (inadequate secretion of intrinsic factor with subsequent reduction in vitamin B12 absorption).
(2) Vitamin B12 is used after partial or total gastrectomy to mitigate the loss or reduction of intrinsic factor synthesis.
(3) Administration of vitamin B12 is used to replace vitamin B12 deficiency caused by dysfunction of the distal ileum with defective or absent absorption of the intrinsic factor–vitamin B12 complex.
(4) Administration of vitamin B12 is necessary in patients with insufficient dietary intake of vitamin B12 (occasionally seen in strict vegetarians).
*Adverse effects of vitamin B12*
are uncommon, even at large doses. Hypokalemia and thrombocytosis can occur upon conversion of severe megaloblastic anemia to normal erythropoiesis with cyanocobalamin therapy
are uncommon, even at large doses. Hypokalemia and thrombocytosis can occur upon conversion of severe megaloblastic anemia to normal erythropoiesis with cyanocobalamin therapy
*_Treatment of pernicious anemia Administration of vitamin B 12 by injection and not by mouth (because most cases occur secondary to lack or the intrinsic factor)._*
*2. Folic acid (vitamin B9) (Folacin, leucovorin)*
*2. Folic acid (vitamin B9) (Folacin, leucovorin)*
*Source* in food – yeast, egg yolk, liver and leafy vegetablesFolic Acid (F.A.) is absorbed in the small intestines. F.A. is converted to tetrahydrofolate by dihydrofolate reductase.
*Folic Acid deficiency* (F.A. Deficiency) is also called Will’s Disease. Deficiency may produce megaloblastic anemia; neural tube defect in fetus.
*Therapeutic Uses of Folic Acid*
1. Megaloblastic Anemia due to inadequate dietary intake of folic acid Can be due to chronic alcoholism, pregnancy, infancy, impaired utilization: uremia, cancer or hepatic disease.
1. Megaloblastic Anemia due to inadequate dietary intake of folic acid Can be due to chronic alcoholism, pregnancy, infancy, impaired utilization: uremia, cancer or hepatic disease.
2. To alleviate anemia that is associated with dihydrofolate reductase inhibitors. i.e. Methotrexate (Cancer chemotherapy), Pyrimethamine (Antimalarial)Administration of citrovorum factor (methylated folic acid) alleviates the anemia.
3. Ingestion of drugs that interfere with intestinal absorption and storage of folic acid.
3. Ingestion of drugs that interfere with intestinal absorption and storage of folic acid.
Mechanism to point 3 above- inhibition of the conjugases that break off folic acid from its food chelators. Ex. – phenytoin, progestin/estrogens (oral contraceptives)
4. Malabsorption – Sprue, Celiac disease, partial gastrectomy.
5. Rheumatoid arthritis – increased folic acid demand or utilization.
More about folic acid👇🏿👇🏿
a. Folic acid is composed of three subunits: pteridine, para-aminobenzoic acid (PABA), and one to five glutamic acid residues.
(1) Folic acid typically occurs in the diet in a polyglutamate form that must be converted to the monoglutamyl form for absorption. Most folate is absorbed in the proximal portions of the small intestine and is transported to tissues bound to a plasma-binding protein. Folic acid requires reduction by dihydrofolate reductase to the active metabolite methyltetrahydrofolate.
(2) Leucovorin is a racemic mixture of the d/l stereoisomers of 5-formyltetrahydrofolic acid. It does not require metabolism by dihydrofolate reductase.
b. The cofactors of folic acid provide single carbon groups for transfer to various acceptors and are essential for the biosynthesis of purines and the pyrimidine deoxythymidylate. A deficiency in folic acid results in impaired DNA synthesis; mitotically active tissues such as erythroid tissues are markedly affected.
c. Catabolism and excretion of vitamin B9 are more rapid than that of vitamin B12; hepatic reserves are sufficient for only 1–3 months.
d. Folic acid and leucovorin are usually administered orally.
e. Folic acid is used to correct dietary insufficiency (commonly observed in the elderly), as a supplement during pregnancy to decrease the risk of neural tube defects, during lactation, and in cases of rapid cell turnover, such as hemolytic anemia. Leucovorin may be used to reverse the effects of the folate antagonists methotrexate, pyrimethamine, and trimethoprim.
a. Folic acid is composed of three subunits: pteridine, para-aminobenzoic acid (PABA), and one to five glutamic acid residues.
(1) Folic acid typically occurs in the diet in a polyglutamate form that must be converted to the monoglutamyl form for absorption. Most folate is absorbed in the proximal portions of the small intestine and is transported to tissues bound to a plasma-binding protein. Folic acid requires reduction by dihydrofolate reductase to the active metabolite methyltetrahydrofolate.
(2) Leucovorin is a racemic mixture of the d/l stereoisomers of 5-formyltetrahydrofolic acid. It does not require metabolism by dihydrofolate reductase.
b. The cofactors of folic acid provide single carbon groups for transfer to various acceptors and are essential for the biosynthesis of purines and the pyrimidine deoxythymidylate. A deficiency in folic acid results in impaired DNA synthesis; mitotically active tissues such as erythroid tissues are markedly affected.
c. Catabolism and excretion of vitamin B9 are more rapid than that of vitamin B12; hepatic reserves are sufficient for only 1–3 months.
d. Folic acid and leucovorin are usually administered orally.
e. Folic acid is used to correct dietary insufficiency (commonly observed in the elderly), as a supplement during pregnancy to decrease the risk of neural tube defects, during lactation, and in cases of rapid cell turnover, such as hemolytic anemia. Leucovorin may be used to reverse the effects of the folate antagonists methotrexate, pyrimethamine, and trimethoprim.
*It is important for us to know the Mechanism for Peripheral Neuropathy*
👇🏿👇🏿👇🏿
Cobalamin is a cofactor for the enzyme Methylmalonyl-CoA mutase which converts methylmalonyl-CoA to succinyl-CoA. Succinyl-CoA enters the Krebs cycles and goes into nerves to make myelin. If no Vitamin B12, methylmalonyl-CoA goes on to form abnormal fatty acids and causes subacute degeneration of the nerves.
👇🏿👇🏿👇🏿
Cobalamin is a cofactor for the enzyme Methylmalonyl-CoA mutase which converts methylmalonyl-CoA to succinyl-CoA. Succinyl-CoA enters the Krebs cycles and goes into nerves to make myelin. If no Vitamin B12, methylmalonyl-CoA goes on to form abnormal fatty acids and causes subacute degeneration of the nerves.
*Only B12 can correct this problem*.
~~ Finally 😊
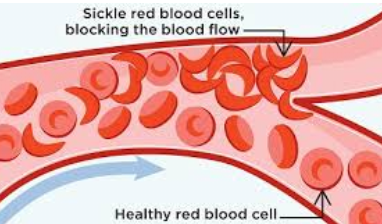
*5.Sickle cell anemias*
1. Hydroxyurea has been shown effective in reducing painful episodes by about 50%; the necessity of blood transfusions was also shown to be reduced. Hydroxyurea increases the production of fetal hemoglobin, which makes red cells resistant to sickling and reduces the expression of adhesion molecules such as L-selectin.
2. Pentoxifylline (Trental) is a synthetic dimethyxanthine structurally similar to caffeine. The actions of pentoxifylline include increased erythrocyte flexibility and decreased blood viscosity. It is commonly used to treat intermittent claudication. Pentoxifylline appears to inhibit erythrocyte phosphodiesterase, which causes an increase in erythrocyte cyclic adenosine 5′-monophosphate activity and an increase in membrane flexibility
This is a detail about ANAEMIA.
This is a detail about ANAEMIA.
Comments
Post a Comment
Real education enhances the dignity of a human being and increases his or her self-respect. If only the real sense of education could be realized by each individual and carried forward in every field of human activity, the world will be so much a better place to live in.
- A. P. J. Abdul Kalam -